











Nutrition Program to Chepang in Dhusa VDC, Syadul, Dhading District
INTRODUCTION
The World Health Organization estimates that malnutrition accounts for 54 percent of child mortality worldwide, about 1 million children. Even mild degrees of malnutrition double the risk of mortality for respiratory and diarrheal disease mortality and malaria. This risk is greatly increased in more severe cases of malnutrition. There are three commonly used measures for detecting malnutrition in children: stunting (extremely low height for age), underweight (extremely low weight for age), and wasting (extremely low weight for height). These measures of malnutrition are interrelated, but studies for the World Bank found that only 9 percent of children exhibit stunting, underweight, and wasting. According to a 2008 review an estimated 178 million children under age 5 are stunted, most of whom live in sub-Saharan Africa. A 2008 review of malnutrition found that about 55 million children are wasted, including 19 million who have severe wasting or severe acute malnutrition. Measurements of a child’s growth provide the key information for the presence of malnutrition, but weight and height measurements alone can lead to failure to recognize kwashiorkor and an underestimation of the severity of malnutrition in children.
Proper nutrition is a powerful good: people who are well nourished are more likely to be healthy, productive and able to learn. Good nutrition benefits families, their communities and the world as a whole.
Undernutrition is, by the same logic, devastating. It blunts the intellect, saps the productivity of everyone it touches and perpetuates poverty.
As UNICEF documented in its 2013 report,‘Improving Child Nutrition: The achievable imperative for global progress’, the scope of under nutrition goes beyond the crises we see in the headlines. Stunting affects 165 million children under five years old – one out of every four.
Stunting - or low height for age - traps people into a lifelong cycle of poor nutrition, illness, poverty and inequity. The damage to physical and cognitive development, especially during the first two years of a child’s life, is largely irreversible. A child’s poorer school performance results in future income reductions of up to 22 per cent on average. As adults, they are also at increased risk of obesity, diabetes and cardiovascular disease.
In 2012, an estimated 25 per cent of children under five years of age were stunted globally, or 162 million children, which represents a 37 per cent decrease from an estimated 257 million in 1990. However, a new Lancet article on nutrition from 6 June 2013 shows that progress is not fast enough, so what is needed now is strong, global commitment and leadership to accelerate efforts.
There are many compelling reasons to increase efforts. A group of leading economists, theCopenhagen Consensus, has consistently confirmed that taking action on undernutrition is the single most important, cost-effective means of advancing human well-being. Thus would accelerate the achievement of the Millennium Development Goals, save lives and should be a top global priority.
UNICEF is a key partner in the major global initiative called the Scaling Up Nutrition (SUN) movement, which is bringing much needed focus and investment for nutrition in a number of countries. In addition, UNICEF is committed both to working in and convening partnership across all sectors of society with governments, UN organizations, the private sector and civil society.
Proper nutrition helps give every child the best start in life. UNICEF is committed to scaling up and sustaining coverage of its current high-impact nutrition interventions in the programme areas of: (1) Infant and Young Child Feeding; (2) Micronutrients; (3) Nutrition Security in Emergencies; and (4) Nutrition and HIV/AIDS. UNICEF is committed to a life-cycle approach, to using partnerships and to creating and enhancing integrated interventions to maximize effectiveness, such as combining vitamin A supplementation with other accelerated child survival interventions through Child Health Events.
INTRODUCTION OF DHADING DISTRICT,DHUSA VDC AND CHEPANG
DHADING DISTRICT
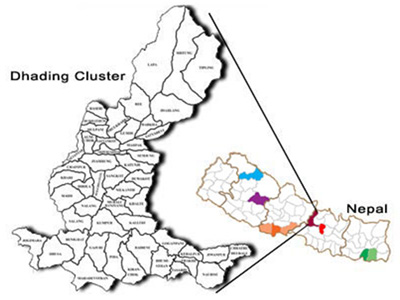 The Dhading district extends from 27º 40' N to 28º 14' N Latitude and 84º E to 85º 1' East longitude and is surrounded by Gorkha district in the west, Kathmandu and Nuwakot the east, Makawanpur and Chitwan in the south and Rasuwa district in the north. The north frontier is also bordered with Tibet Autonomous Region of the Peoples Republic of China. The shape of the district is like a military boot and represents different agro-climate zone comprising of valley, Tars (flat land) to middle hills and high hills. It has a total area of 192,487 hectare.
The Dhading district extends from 27º 40' N to 28º 14' N Latitude and 84º E to 85º 1' East longitude and is surrounded by Gorkha district in the west, Kathmandu and Nuwakot the east, Makawanpur and Chitwan in the south and Rasuwa district in the north. The north frontier is also bordered with Tibet Autonomous Region of the Peoples Republic of China. The shape of the district is like a military boot and represents different agro-climate zone comprising of valley, Tars (flat land) to middle hills and high hills. It has a total area of 192,487 hectare.
The elevation ranges from 488 meter to 7409 meter above mean sea level. The highest peak of Ganesh Himal is 7409 meter high located most part of the district at Tipling VDC. The climate conditions are representative for a hill district in the Central Development Region of Nepal. The major climate zones found in Dhading district include the following:
- Sub Tropical Zone in areas below 1000m.above mean sea level with the annual average temperature of above 20º C.
- Temperature Zone in altitude between 1000-3000m.MSL with annual average temperature between 10º - 20ºC.
- Alpine Zone in greater than 3000 m above MSL with average temperature of less than 10º C.
- The average annual rainfall as recorded at Dhading Besi station is 2121.2 mm. The rainfall pattern is different due to altitudinal variations. The rainy season is the longest at VDCs located at eastern area while it is slightly shorter in western and northern part. Usually, rainfall is in from of snow in high altitudes of Lapa, Sertung, Tipling and Jharlang.
The district is administratively divided into 13 lakhs that consist of 50 VDCs in total. Each VDC is divided into 9 wards. Each ward comprised of 1 to 4 clusters or hamlets depending upon the size of the population.
It is also one of the most backward districts which stands in 41st rank in Human Development Index (HDI) among 75 districts of Nepal. The district is entirely composed of the villages with fifty Village Development Committees with no municipalities. The district has poor development infrastructures like roads, electricity, and others. The district statistic shows only 39% of the population in the district has access to clean drinking water and only small percentages of them have sanitary toilets. Most of the populations are based on subsistent agriculture and have low income for basic livelihood. It is commonly observed that large percentage of the youth populations are unemployed who are going for foreign employment nowadays.
There are 380,369 populations with a growth rate of 1.97 and an average family size is 5.4. The district has only 43% adult literacy rate where female literacy rate is considerably lower (33.81%) compared to the male (53.69%). The district has high percentage (over 35%) of poor and marginalized ethnic population. The main marginalized ethnic communities in the district are Tamang (19%), Dalits (9%), Chepangs (3%), and Kumals (1.2%). These ethnic communities have poorer socio-economic condition far behind the average population of the district.
The district is behind in health status compared to the national level. Although the health indicators are significantly improving over the years, the district is still behind in some of the key indicators. The child mortality rate (CMR) is 101.7/1000 and Infant Mortality Rate (IMR) is 91.8/1000 and average life expectancy is only 49.5 years. The health status of the marginalized communities is much worse than the average district situation. Occurrence of preventable and communicable diseases like skin diseases, diarrhea, gastritis and intestinal worms, typhoid and ear infection among the top ten diseases reflects poor health situation of people in the district.
DHUSA VDC
The Dhusa VDC is situated southeast of the Charaundi Bazar at the Prithivi Highway. There are no alternatives besides walking on foot to reach the site and it requires 6-7 hrs walking from the road head. Chepangs, considered as primitive and the most backward ethnic groups of Nepal are the ancient settlers in the area. They are living in the highly fragile and difficult terrains close to the forest and the households are highly scattered. The total household number of the VDC is 1361 (CBS 2012) out of which only around 450 households are of Chepang (Chepang district profile, Dhading 2006).
CHEPANG
Chepangs whose population is about 52, 000 (0.23% of total population) with only 13.9 per cent literate are considered to be one of the most primitive communities of Nepal (CBS 2003). They are distributed in six districts of Nepal’s 75 districts. However, the population is concentrated to Chitwan, Makawanpur, Dhading and Gorkha (Chepang Voice 2006). Chepang has their own language but most of them can speak Nepali as well. Chepangs are traditionally hunters who use bows and arrows and hunting dogs. As hunting is an important source of their livelihood, two words are central in their language: che, dog, and pang, arrow (Manandhar 2002).
Chepangs have lived semi-nomadic depending on shifting cultivation farmingsystems supplemented with hunting and gathering. For centuries, Chepang have been a forest tribal community with their own mythology, customs, rituals and life style (Manandhar 2002). They are influenced by both Hinduism and Buddhism and their main festival is Nwagi Puja (which is performed on a Tuesday during third week of Bhadra (August - September). Moreover, the economy of the Chepang is forest and stream-based with simple and indigenous technology. The major crops are Maize (Zea mays) and Finger Millet (Eleusine coracana). On average their own production is sufficient for about 5 months per year and only one percent of the Chepang have sufficient food for the whole from their own production (Gurung 2006). The rest of the months they depend on wild and uncultivated foods and wage labour work to meet their food demand (Regmi et al. 2006). The land tenure is the biggest problem among the Chepang communities as most of the shifting cultivators do not have land registration certificate (Regmi et al. 2003).
RATIONAL OF THE PROGRAM/HEALTH SITUATION OF CHEPANG
The district is behind in health status compared to the national level. Although the health indicators are significantly improving over the years, the district is still behind in some of the key indicators. The child mortality rate (CMR) is 101.7/1000 and Infant Mortality Rate (IMR) is 91.8/1000 and average life expectancy is only 49.5 years. The health status of the marginalized communities is much worse than the average district situation. Occurrence of preventable and communicable diseases like skin diseases, diarrhea, gastritis and intestinal worms, typhoid and ear infection among the top ten diseases reflects poor health situation of people in the district. Mainly, the Chepang children are suffering from Malnutrition due to the lack of proper knowledge of nutrition and hygienic environment maintenance for the children. They are suffering from the following diseases:
- fatigue and low energy
- dizziness
- poor immune function (which can hamper the body's ability to fight off infections)
- dry, scaly skin
- swollen and bleeding gums
- decaying teeth
- slowed reaction times and trouble paying attention
- underweight
- poor growth
- muscle weakness
- bloated stomach
- osteoporosis, or fragile bones that break easily
- problems with organ function
- problems learning
The causes related to Malnutrition
- Lack of proper nutritious food
- Traditional understanding of food
- Short time gap in between two consequent children (1-2 years)
- Lack of Knowledge of Family Planning
- Lack of proper parental caring
- Low economic status
- Lack knowledge and education
- Geographical difficulties area
In district, Chepangs are living in 10 VDCs. Out or 10 VDCs, we selected the Dhusa VDC for initiation of the program.
| District: | Dhading |
| VDC: | Dhusa |
| Ethnic Group: | Chepang |
| Population: | 1361 |
| Households: | 450 |
| Expected No. of Children: | 600 |
| Pregnant women: | 80 |
| Time Duration of Project: | 12 Months |
OBJECTIVES
- To access the knowledge of Nutrition to the mothers
- To empower the mothers how to make nutritious food for the children.
- To supply the nutritious food to the pregnant mother
- To supply the nutritious food to the children (Infants to the age of 6)
PROGRAMS FOR THE CHEPANG CHILDREN
The following programs need to be implemented to improve the Nutrition Condition of Chepang Children:
- Survey of Chepangs find out the name, age, sex, health condition, birth-rate, diseases, status of nutrients and socio-economic profile.
- Organizing the awareness campaign for each ward to the mothers how to keep their children tidy and healthy
- Training and Orientation Programs for making nutritious food by using local resources and food available.
- Supply of Nutritious food to the Pregnant women and deliver the value of Nutrition, aware them (door to door campaign)
- Supply of Nutritious food to the Children (Infants to the age of 6).
- Orientation for School Children about Health and Hygiene, and importance of Nutritious food in schools.
- Monitoring and Supervision after implementation of Program
EXPECTED OUTPUT
- 90% mothers will be followed how to make their children tidy and healthy
- 90% mothers will be able to make nutritious food by using local food to their children.
- The mothers or family members will be continuing to keep their children tidy and healthy and making nutritious food by using local resources.
- The school going children will be aware about their health and hygiene, and importance of Nutrition.
- The pregnant women will be able to take care their health in proper way.
- More than 80% malnutrition problem will be reduced.
SUSTAINABILITY
The teams of HOMES Nepal not only conduct the programs for the Chepangs, it also seeks for the sustainability of programs. The programs deal with the empowerment of the Chepangs and after completion of projects they will be aware and able to prepare the nutritious food themselves by using the local food produced in their local area. They will be able to know the nutritious value for the growth of children and importance of nutrition in pregnant and new born babies. In the training session, HOMES Nepal team will also deliver and empower the livelihood programs and ideas related to their skill and knowledge. The homes Nepal team will monitor in regular basis.
CONCLUSION
Malnutrition affects people of every age, although infants, children, and adolescents may suffer the most because many nutrients are critical for normal growth and development. Older people may develop malnutrition because aging, illness, and other factors can lead to a poor appetite, so they may not eat enough.Malnutrition is well recognized as a widespread health problem with consequences that are both acute and, even more often, long-term. Both acute and underlying effects contribute to mortality, either directly or indirectly (through weakened defenses against other diseases such as malaria, respiratory, or diarrheal diseases). However, the long-term effects, especially from nutritional deficits early in life, on children who don't die, but have their development impaired, may exceed even the troubling mortality.Malnutrition harms both the body and the mind. The more malnourished someone is — in other words, the more nutrients that are missing — the more likely he or she is to have problems.
Download this page as MS-WORD file | Download this page as PDF file